Thursday, February 23, 2006
Thursday, February 23, 2006
Volunteers Rock! The last year has been an amazing journey building this new clinic.we've managed to sustain ourselves thru fair prices, support three part-time practitioners and do a lot of high quality, integrated health care. none of it would have been possible without the help o our volunteers. we have volunteers working with us on two different levels - massage therapists and receptionists. Massage Therapists: Jennifer and Matthew have both volunteered their time with us to care for very poor, stressed out people, most of whom have never had body work in their lives. we send them whole families! they have both made time each week for 3 hours and we are so appreciative, as are our patients. the best story i've heard so far is a woman who came in thinking she had gall bladdder disease, months of terrible abdomenal pain, and after a single massage session, she had lost 20 years of age, her pain had dissolved, and she was ready to dance. :> Receptionists: Bianca, Glenda, Camila, Laura and Lorenzo are our volunteer receptionists. They each give 2-4 hours per week hanging out in the clinic with us, answering phones, greeting the patients, and learning how to take vital signs, give shots, recognize sick people, and understand the funky pricing/injustice in the health care world. Many of our volunteers are pre-med or pre-nursing and very eager to learn all aspects of clinical medicine. And each brings their own flavor and knowledge that helps our patients - from herbs to WIC to preventive health. Work-Study While i'm at it, i need to say something about our two work-study students. They aren' volunteers, but their diverse services are indispensible - from reception to health literacy projects to coordination of donations. Ocelotl has been with us for about 5 months, has brought a level of professionalism and compassion to the job, and has helped us develoandrup an understanding of how to navigate the local lab to get our patients the best prices. Rose just started last week. She has a strong interest in nutrition and natural medicine. The Family Practice Office is blessed to be part of a growing team of creative, dedicated people at all phases and stages of education. andru
posted by andru |
2/23/2006 11:12:00 AM |
(0) comments
|  
Tuesday, February 21, 2006
HSA's: a great way to burden individuals & govt; I mean, consumer driven health care, yeah!
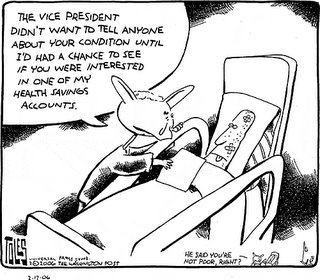 "To summarize, I estimate that the President’s budget proposals will cost almost $12 billion dollars per year if fully phased in. I estimate that these proposals will on net raise the number of uninsured (by 600,000 persons), as those left uninsured through firm dropping of insurance exceed those who gain insurance through taking up tax-subsidized high-deductible plans attached to HSAs." (source: Jonathan Gruber's CBPP/MIT study) "To summarize, I estimate that the President’s budget proposals will cost almost $12 billion dollars per year if fully phased in. I estimate that these proposals will on net raise the number of uninsured (by 600,000 persons), as those left uninsured through firm dropping of insurance exceed those who gain insurance through taking up tax-subsidized high-deductible plans attached to HSAs." (source: Jonathan Gruber's CBPP/MIT study)
And from the press release of the study: The analysis, conducted by Jonathan Gruber of M.I.T., projects that while 3.8 million previously uninsured people would gain health coverage through HSAs as a result of the President's proposals, 4.4 million people would become uninsured because their employers would respond to the new tax breaks by dropping coverage and they would not secure coverage on their own. The net effect would be to increase the number of uninsured Americans by 600,000. "The Administration estimates that its HSA-related tax proposals would cost $156 billion over the next ten years, which would worsen the nation's fiscal problems," Robert Greenstein, the Center on Budget and Policy Priorities' executive director, noted. "Professor Gruber's study raises very serious questions about the wisdom of these proposals."... These proposals would eliminate all tax advantages for employer-sponsored coverage (as compared to coverage purchased in the individual health insurance market). Those tax advantages were designed to encourage employers to provide insurance to their workers. As a result, some employers -- typically, small business owners -- would respond to the new HSA tax breaks by dropping coverage for their workers or (in the case of new businesses) electing not to offer coverage in the first place... To estimate the impact of these proposals on health coverage, Professor Gruber employed a micro-simulation model that is very similar to models used by the Congressional Budget Office, the Congressional Joint Committee on Taxation, and the Treasury Department. His findings include: -- Under the proposed tax breaks, the number of people with individual health coverage would increase by 8.3 million when the proposals were fully in effect. Some 3.8 million of these people would previously have been uninsured; about 4 million of them would have switched from employer-sponsored coverage to individual coverage coupled with an HSA; and 500,000 would previously have received coverage through Medicaid. -- Some 8.9 million people would lose employer-sponsored coverage as a result of the tax breaks. About half of them -- 4.4 million people -- would become uninsured, while another 4 million would switch to individual coverage coupled with an HSA, and 500,000 would enroll in Medicaid... Adding to the concerns that Professor Gruber's paper raises, Greenstein said, is the strong probability that the currently uninsured people who would be most likely to gain coverage as a result of the Administration's proposals would be relatively healthy, since they would best be able (with the help of the new tax subsidies) to obtain affordable coverage in the individual market. In contrast, the people most likely to become uninsured would be less-healthy employees in small businesses that dropped coverage, since less-healthy people have the most difficult time obtaining affordable coverage in the individual market.
posted by Unknown |
2/21/2006 09:42:00 PM |
(0) comments
|
Thursday, February 09, 2006
Hi my name is Sri - I am new to this experiment in blogging medicine. I am in residency with Anjali and homies with Andru from a Patch Adams gathering last year. I spent last April in a refugee camp for Tibetans in India. Here is an essay I wrote about the experience. Hopefully, it isn't too long to hold your attention.
- Sri
The largest Tibetan refugee colony in the world lies five hours from where I spent the summers of my childhood at my grandmother’s house in Bangalore,India. Neither my mother nor my father nor most of my Indian relatives who grew up in Bangalore knew of its existence despite the fact that it houses over 10,000 refugees. Half of the residents are Buddhist monks and nuns. I first heard about the colony when I decided to spend a part of my final year in medical school abroad inIndia. I wanted to experience rural medicine inIndia and understand the barriers that prevented the poor from receiving adequate health care. I also liked the idea of returning to my ancestral home stateof Karnataka, and improving my Kannada. The hospital was attempting to serve the Tibetan refugee population and desperately needed medical volunteers. I was unsure how much Kannada I would use but the location was rural, in Karnataka, and would allow me the chance to work with a refugee population that had been in India for generations.
--- I spent the first night in Bangalore at my cousin’s house and the next day left early for Bylakuppee. After passing through the smoggy, congested streets ofBangalore, we entered village after village where crowds poured out into the streets and hot dust mixed with the hum of the simultaneous Kannada spoken soft and loud and almost sung in every corner store shop. After about the four hundredth tea stall and street food daba, we reached a stretch of the greenest forests and farmlands. Somewhere in that stretch of farmland and open green road the climate changed from the sulky suffocating heat of April in South India toa cool about to rain comfortable. And somewhere along that stretch of road the color of the faces changed from a rich, beautiful brown of my familiar knowing toa lighter yellowish East Asian undertone. The eyes changed. Just as the faces changed, there rose out ofthe green earth four or five massive Buddhists temples and universities in a row spread out and separated by about ½ mile each. ---- I found out quickly that I had entered a place with entirely different notions about life purpose and productivity. Soon after I arrived I pointed out to a monk that a mosquito was sucking his blood. He nodded in acknowledgement and said something brief about the accumulation of merit and allowing another being to nourish itself off your own. (Luckily, we were in a region where the prevalence of malaria is low). The second day I was there, a monk took me to the local Indian restaurant. A fly fell into my daal. The monk’s reaction took me by surprise. I wrote this poem about it. ----- For my friend who says the way the world works has broke her heart: good news from the subcontinent. Living with the monks study #1 ---- There are those who When a fly drops Plop! into yellow daal it is not their bowl of food they worry about. It is the fly and her wings The ability of fire and spice To sear wings And with so much kindness They place the fly in their palm Unfold a white creased napkin Clean the wings and the space Between the wings with water rinse away Any hot yellowness Place the fly gentle On the edge of the table Until by the end
Of our meal The fly has flown made her way Back into the world ---- I worked in fourth camp where there were over 3000 monks and 600 nuns, mostly between the ages of 5 and25. They attended the large Buddhist school in the colony which did not teach math and science, onlyBuddhist philosophy. Children were separated by their proficiency in Tibetan. As a result 15 year olds are placed side by side with seven year olds. Most of the monks and nuns came from Nepal, Bhutan, Darjeeling,Sikhim, and Tibet. They came for a variety of reasons. Some of the older teenagers came out ofconviction and interest. The younger children were sent by traditional Buddhist families who believed it was auspicious to have at least one family member become a monk. Still other families were very poor and knew that sending their child to a monastery or nunnery would at least guarantee that they would receive three meals a day.
To go along with my many new experiences, the hospital was like none I had ever seen. There was no doctor. None at all. The doctor who had been there for a few months was a retired ENT doctor who wanted to make some extra money at the camp. He was from the city and did not stay past two months. Without a steady physician, the hospital had not been useful for the monastery or nunnery trying to take care of their population. --------- As the hospital struggled to get off the ground, Sherap Lama, a 30 year old monk from Sikhim decided some form of health care was necessary for the young monks. He was a schoolteacher at the Buddhist school and saw so many oozing pus filled ears, belly aches, bald spots and six children die from unknown causes that he attempted to start a clinic. About a year and a half before I came to the colony, he obtained a copy of the book Where There Is No Doctor and studied it. He raised money to buy some medical equipment and medications to treat the young monk school children. His clinic consisted of keeping semi-hygienic conditions in the monastery. Boys were clumped together 14-15 in a small room to sleep. Monks or not, groups of young boys with parents nowhere insight do not willingly wash. Before Sherap set up a spare room as a clinic, the community would say the stray dogs looked better than the children.
Sherap made enough progress in his project that the nuns soon grew interested. Sherap taught Ani Dichen, a young nun from Nepal about what he learned and she soon started a similar clinic for the 600 nuns. -------- I spent my mornings at the monk makeshift clinic and my afternoons at the nunnery clinic. At seven in the morning the young monks would line up to see me. In my first week there at the clinic I met a young 14 year old boy, coughing up blood. I soon realized that crowded sleeping conditions caused the quick spread of serious ailments like tuberculosis. More and more boys with chronic coughs and blood tinged spit started to present themselves. This meant that I had to come up to speed on the protocol for treating TB patients in India. I learned of the WHO recommended plan called the RevisedNational Tuberculosis Control Programme which was orchestrated throughout the country by the Indian government and financed with a loan from the World Bank. ----------- The closest government distribution of medications was about 10 minutes away by auto, in first camp. I immediately went to speak with theIndian government doctor in charge of the local program about the high rates of tuberculosis I hadnoticed. He knew the reality of fourth camp well. He was aware of a 22 year old monk who had been left partially paralyzed and that TB had spread to his spine. He was well aware six other monks had started treatment after they began coughing up blood and another three were dead of an “unidentified sickness”. These outbreaks took place within a year in a population of 3000. He knew that treatment in fourth camp was sometimes sporadic and continued isolation of the infected monks was not maintained with regularity. -------- With highly effective treatment so close by it seemed unacceptable to me that so many cases of tuberculosis should go undiagnosed and not treated properly. He stated that the Tibetans were non-compliant by nature and difficult to keep track of since they regularly travel through India and between different Tibetan colonies all over the country.The reality, however, was that although the government had provided state of the art treatment there was no doctor or health care worker on site in camp four to diagnose TB. Sherap and Ani Dichen had been extremely proactive in starting their own makeshift clinics. No government program was in place to train them to recognize the symptoms of TB. The result was that many monks would continue to go undiagnosed until they coughed up blood and came forward on their own accord. Meanwhile, before getting treatment they were likely to spread TB to those sleeping less than two feet away from them. -------- If a monk can show so much concern for the fate of a fly surely we can muster up enough courage to stop the death of those dying needlessly in front of our eyes. As my short month came to an end it became obvious that in this historical moment the requirements of being a real deal effective doctor goes up hundredfold. -------- Doctors must understand structural inequalityand their underpinnings. We must understand the politics of funding projects, where the money comes from and where it is being funneled towards, and to what end? We must start one on one, patient by patient and expand out to include so many things we never thought were medicine. Poverty, race, class. WorldBank funding practices. If only out of necessity, because our patients’ lives depend on it. We must tell the stories again and again of who died and what commitment financial or otherwise could have prevented it. We must understand who is vulnerable and why? Who becomes sick and why? We must strive to be doctors and advocates. Doctors and organizers. Doctors and policy makers. Doctors and journalists. --------- Of so much good news from the subcontinent, the status of TB in the Tibetan colony is not one of them. But the key, I think is to make it news. If it becomes news, maybe it will turn good. As the poet June Jordan says “We are the ones we are waiting for.” There are so many Sherap Lama’s and Ani Dichen’s who are ready and willing. I hope to be among them.
posted by srijeeva |
2/09/2006 10:54:00 AM |
(4) comments
|
Monday, February 06, 2006
Clinic Vignettes February 11, 2006a 37yo man presented with signs and syptoms of stroke, right arm weakness, right leg heaviness and a slight change in speech. this is very unusual in young people. the first day he presented last week, i was totally confused and didn't put the story together until after he left. he had a few other complaints and i didn't pick up on the leg and speech changes until his second visit. the first night after he left, i was thinking alot about him and started getting more and more concerned. we spoke by phone the next day and my suspicions were confirmed with deeper questioning. he had symptoms for almost two weeks so he was well outside the 3 hour time period to try to do anything about a stroke urgently but it never makes you happy as a doctor when you miss something important. back in my clinic at his second visit, we did a thorough review of systems and picked up a bleeding tendency and a smoking history as the only two risk factors i could find. so here ends clinical medicine and now starts this mans journey into the perpetually painful world of trying to get healthcare when uninsured for a complicated illness. turns out this man is undocumented. he was trying to be responsible and was a few weeks ago from his work insurance kicking in... with the urgency of the situation, we can't wait a few weeks to i had no choice but to send him to the public hospital ER for an immediate workup which will no doubt nail this man with a pre-existing condition prohibiting his imminent insurance from taking effect. this man has bigger worries, but this financial piece is going to be a painful thorn in his side. he has lost significant function of his left hand and will no longer be able to do the construction work that was supporting him and his family. and he will not be eligible for disability as a non-citizen. now for all you people reading this who immediately think - "well, so what, why doesn't he just go back to his own country," let me run a few ideas by you. immigrants make up the majority of this country, every one of us, except for the "First People's," also known as Native Americans, are immigrants. so who is calling who illegal. secondly, many Mexicans in particular have made the southwest their home for thousands of years, crossing what is now a border as naturally as any of us would cross a state line. many Mexicans are Indigenous and have historical roots long predating the formation of the United States of America. That's just a little reminder of whose land we stand on, and a brief history lesson. Now fast forward to the present moment where we live in the comfortable illusion that this country is Ours. Even in that case, it cannot be denied that "illegal" immigration is a huge part of what makes this nation so great. our fields, restaurants, contruction sites, music, culture, house cleaning, etc are fueled by the continual influx of illegal immigrants, people drawn to this land by the hunger in their bellies and the very real promise of businesses and people who demand their cheap labor. if you are sitting there on your couch having some stiff opinion about people you don't know, about economics you don't understand, then please, turn off teh computer, do some traveling, learn a second language, study macro-economics and history, and then, let's talk. (By the way, i got a call from the family after two days in the hospital, this man didn't have a stroke, he had cancer of the brain. they found four separate lesions in his head. the family is awaiting the biopsy results at this moment.) -------------------------------- a 28yo man comes to the clinic with right sided eye pain and redness for three days. he does landscaping and was out in the wind when a bunch of dirt got in his eye. on flourosceine/woods lamp exam he had a large corneal scratch and a piece of dirt, small, sticking into his cornea. the dirt wouldn't come out with irrigation. luckily i had purchased a Nikon slit lamp which is a microscope for examining the surface of the eye. it's a really cool tool. i picked it up for $150 used from a local eye doctor who had a newer electronic one. they usually run for about $5000 or more. with the slit lamp and some courage, i was able to remove the speck of dirt saving this guy a visit to the ER for a cost of $500-2000. a note for other docs starting up clinics - you can make your own woods lamp for about $10 instead of $300. just buy a regular bulb lamp, portable is best, and use a "black light" bulb. works great. we wound up charging the man $50 for the visit and procedure. he left very happy and promised to use his safety glasses next time. andru
posted by andru |
2/06/2006 04:50:00 PM |
(0) comments
|
Thursday, February 02, 2006
Clinic Vignettes - February 1, 2006 Yesterday a patient called from an ER. He had been there a few hours already with a cut on his hand and was looking at a long wait and a huge bill. We were open so he abandoned ship, left the ER, and with his hospital bracelet still on, came over to the clinic for stitches. 20 minutes, $40 and 4 stitches later, he was on his way home... it doesn't have to be that complicated. A pregnant woman showed up at the clinic around 6 weeks gestational age. she was complaining of passing a clot vaginally. no cramping. she was concerned that she was having a miscarriage. she had already scheduled her first prenatal appointment, but it wasn't for 6 more weeks at the local hospital clinic for poor women. noone educated her that she could go there sooner if she had a problem. she was already concerned that the public hospital ER would not treat her well thru bad experiences of friends, neighbors and her husband, so she refused to even consider going there. With an exam and the ultrasound i was able to verify that she still had a viable pregnancy but was at risk of miscarriage. we are watching and waiting this week to see what nature will do. i've mentioned this previously - Spontaneous miscarriage is one of the most frustrating health policy situations for me as a doctor. pregnant women hope beyond hope for a normal pregnancy and a healthy child. the medical system is geared for maximal cost and reimbursement. uninsured woman have no easy access to urgent care. most private urgent cares charge $150 up front so the ER looks alot more inviting since the bill comes later. Miscarriage early in pregnancy is a natural, often sad, but fairly uncomplicated medical problem that doesn't necessarily need much intervention, and there is NO WAY to medically prevent an early miscarriage. put it all together and you get financial injury compounding emotional distress. it's just not right. can some politician PLEASE take some leadership on this? ths same woman's husband had already had an ER experience for a badly infected big toe. They removed his toe nail for him. guess how much he was charged. $800.00. blows my mind. at what point does it become unethical and/or even illegal to charge someone exhorbitant prices for basic medical services? there is a law called the New Mexico Fair Practices Act that supposedly is there to prevent used car salesmen from ripping off unsuspecting customers. It;s about time to see if this law applies to healthcare as well... these stories just keep on coming. i'm determined to share stories every week now, if nothing else to document the incessant toxicities of our health care system. today a young women came to my clinic with one year of abdominal pain. she had previously had her appendix cut out at the public hospital for the same pain. turned out that the appendix was normal. (as a medical side note, that doesn't particularly bother me. for a surgeon to be sure that they aren't missing any life threatening surgical conditions, they have to have the flexibility to make some mistakes in the direction of unnecessary surgeries to some small degree. in a statistical and complex world, i'd rather have a surgeon make some mistakes like that than be too stringent and make mistakes that cost people their lives.) given all that, the problem in this case is once again, FINANCIAL. this young woman was given a bill of $50,000. did you catch that? $50,000. for removing an appendix. she is a citizen, but for some loophole she didn't qualify for the public hospital financial assistance so she is now paying this bill for the rest of her life. ain't right. perhaps $5,000. it just ain't right. andru
posted by andru |
2/02/2006 04:12:00 PM |
(3) comments
|
|
|
|
| cure this! |
|
We've MOVED! and grown!
Join us at Cure This!...
...where we invite you to create a user account, read, comment, write your own posts. Let's discuss health in its broadest sense, share personal stories, creatively make positive change, and build an online community along the way...
|
|
| what's "to the teeth"? |
|
To the Teeth is a weblog discussing issues of health justice, medicine, race in America,
public health in its broadest sense, healthcare at a local clinic level, and honest discussions around strategies in advocacy. Ok, so it's not so focused, but it's all connected. The regulars who post to this site are:
Anjali Taneja, a resident physician in Family Medicine at Harbor-UCLA in Los Angeles,
California (a recent transplant from the east coast). She also blogs at Los Anjalis and the
Harbor-UCLA Family Medicine Residency blog. She's on the national leadership of the National Physicians Alliance and previously worked as the Jack Rutledge Fellow for Universal Health Care
& Eliminating Health Disparities at AMSA. She dj'ed for several years with the
M U T I N Y dj crew and currently DJs and produces electronic music. (email: movement-at-gmail-dot-com)
and Andru Ziwasimon, a family medicine physician in Albuquerque, New Mexico, and a lead member of the Community Coalition for
Healthcare Access, a diverse group of providers/patients/advocates addressing access issues with the state hospital system, translation and interpretation issues, billing for under and uninsured patients, and other disparities locally.
He created and runs a sustainable and innovative clinic that serves
uninsured patients with quality care and fair prices. He also serves on the leadership of the National Physicians Alliance. (email: aziwa-at-null-dot-net)
and Sri Shamasunder, a resident physician in Internal Medicine at Harbor-UCLA in Los Angeles, CA. He's passionate
about health justice, good music, and spoken word/poetry. (email: elsrizee-at-yahoo-dot-com)
"to the teeth" (idiom):
-> in opposition; directly to one's face
-> completely, fully
-> title of a song by Ani Difranco
-> alotta alliteration
For them RSS lovers (more about rss here), here's the atom site feed for To the Teeth.
|
|
| hot links |
|
Inspiring spoken word from Poetic License
Conversation: Growing up in the Shadow of Chemical Pollution - Michigan and Bhopal
Missing: Minorities in the Health Professions
Angell: The Truth about Drug Companies
Wonderful animation on procrastination!
|
|
| dope orgs/sites |
|
National Physicians Alliance
American Medical Student Association
The Peoples' Institute
Alternet
The Policy Action Network
The Principles Project
Common Dreams
No Free Lunch campaign
Kaiser Family Foundation
Families USA
Consumer Project on Technology
Campaign for a National Health Progam NOW
|
|
| to the teeth archives |
|
12/01/2002 - 01/01/2003
01/01/2003 - 02/01/2003
02/01/2003 - 03/01/2003
04/01/2003 - 05/01/2003
05/01/2003 - 06/01/2003
06/01/2003 - 07/01/2003
07/01/2003 - 08/01/2003
08/01/2003 - 09/01/2003
09/01/2003 - 10/01/2003
10/01/2003 - 11/01/2003
11/01/2003 - 12/01/2003
12/01/2003 - 01/01/2004
01/01/2004 - 02/01/2004
02/01/2004 - 03/01/2004
03/01/2004 - 04/01/2004
04/01/2004 - 05/01/2004
05/01/2004 - 06/01/2004
06/01/2004 - 07/01/2004
07/01/2004 - 08/01/2004
08/01/2004 - 09/01/2004
09/01/2004 - 10/01/2004
10/01/2004 - 11/01/2004
11/01/2004 - 12/01/2004
12/01/2004 - 01/01/2005
01/01/2005 - 02/01/2005
02/01/2005 - 03/01/2005
03/01/2005 - 04/01/2005
04/01/2005 - 05/01/2005
05/01/2005 - 06/01/2005
06/01/2005 - 07/01/2005
07/01/2005 - 08/01/2005
08/01/2005 - 09/01/2005
09/01/2005 - 10/01/2005
10/01/2005 - 11/01/2005
11/01/2005 - 12/01/2005
12/01/2005 - 01/01/2006
01/01/2006 - 02/01/2006
02/01/2006 - 03/01/2006
03/01/2006 - 04/01/2006
04/01/2006 - 05/01/2006
05/01/2006 - 06/01/2006
06/01/2006 - 07/01/2006
07/01/2006 - 08/01/2006
08/01/2006 - 09/01/2006
09/01/2006 - 10/01/2006
10/01/2006 - 11/01/2006
11/01/2006 - 12/01/2006
12/01/2006 - 01/01/2007
01/01/2007 - 02/01/2007
02/01/2007 - 03/01/2007
03/01/2007 - 04/01/2007
07/01/2007 - 08/01/2007
|
|
| poem: history |
|
They caught the peasant walking home from the field.
On the dark road they gagged him and cut off his nose.
This they took to the museum and stuck to the king's noseless statue.
Thus was born the history that is taught in schools.
- Amitava Kumar, "History"
|
|
| Willing to Fight |
|
From Ani Difranco's "Willing to Fight":
"'cause i know the biggest crime
is just to throw up your hands
say
this has nothing to do with me
i just want to live as comfortably as i can
you got to look outside your eyes
you got to think outside your brain
you got to walk outside you life
to where the neighborhood changes"
Excerpts of lyrics to Ani Difranco's poem "Self-evident" (hear her recite this poem on her official website:
yes,
us people are just poems
we're 90% metaphor
with a leanness of meaning
approaching hyper-distillation...
here's a toast to the folks living on the pine ridge reservation
under the stone cold gaze of mt. rushmore
here's a toast to all those nurses and doctors
who daily provide women with a choice
who stand down a threat the size of oklahoma city
just to listen to a young woman's voice
here's a toast to all the folks on death row right now
awaiting the executioner's guillotine
who are shackled there with dread and can only escape into their heads
to find peace in the form of a dream
cuz take away our playstations
and we are a third world nation
under the thumb of some blue blood royal son
who stole the oval office and that phony election
i mean
it don't take a weatherman
to look around and see the weather
jeb said he'd deliver florida, folks
and boy did he ever
and we hold these truths to be self evident:
#1 george w. bush is not president
#2 america is not a true democracy
#3 the media is not fooling me
cuz i am a poem heeding hyper-distillation
i've got no room for a lie so verbose
i'm looking out over my whole human family
and i'm raising my glass in a toast
here's to our last drink of fossil fuels
let us vow to get off of this sauce
shoo away the swarms of commuter planes
and find that train ticket we lost
cuz once upon a time the line followed the river
and peeked into all the backyards
and the laundry was waving
the graffiti was teasing us
from brick walls and bridges
we were rolling over ridges
through valleys
under stars
i dream of touring like duke ellington
in my own railroad car
i dream of waiting on the tall blonde wooden benches
in a grand station aglow with grace
and then standing out on the platform
and feeling the air on my face
give back the night its distant whistle
give the darkness back its soul
give the big oil companies the finger finally
and relearn how to rock-n-roll...
|
|
| subcity |
|
Lyrics from Tracy Chapman's "Subcity"
People say it doesn't exist
'Cause no one would like to admit
That there is a city underground
Where people live everyday
Off the waste and decay
Off the discards of their fellow man
Here in subcity life is hard
We can't receive any government relief
I'd like to please give Mr. President my honest regards
For disregarding me
They say there's too much crime in these city streets
My sentiments exactly
Government and big business hold the purse strings
When I worked I worked in the factories
I'm at the mercy of the world
I guess I'm lucky to be alive
They say we've fallen through the cracks
They say the system works
But we won't let it
Help
I guess they never stop to think
We might not just want handouts
But a way to make an honest living
Living this ain't living
|
|
| the revolution will not be televised |
|
Lyrics from Gill Scott Heron's "The Revolution Will Not Be Televised"
You will not be able to stay home, brother.
You will not be able to plug in, turn on and cop out.
You will not be able to lose yourself on skag and skip,
Skip out for beer during commercials,
Because the revolution will not be televised.
The revolution will not be televised.
The revolution will not be brought to you by Xerox
In 4 parts without commercial interruptions.
The revolution will not show you pictures of Nixon
blowing a bugle and leading a charge by John
Mitchell, General Abrams and Spiro Agnew to eat
hog maws confiscated from a Harlem sanctuary.
The revolution will not be televised.
The revolution will not be brought to you by the
Schaefer Award Theatre and will not star Natalie
Woods and Steve McQueen or Bullwinkle and Julia.
The revolution will not give your mouth sex appeal.
The revolution will not get rid of the nubs.
The revolution will not make you look five pounds
thinner, because the revolution will not be televised, Brother.
There will be no pictures of you and Willie May
pushing that shopping cart down the block on the dead run,
or trying to slide that color television into a stolen ambulance.
NBC will not be able predict the winner at 8:32
or report from 29 districts.
The revolution will not be televised.
There will be no pictures of pigs shooting down
brothers in the instant replay.
There will be no pictures of pigs shooting down
brothers in the instant replay.
There will be no pictures of Whitney Young being
run out of Harlem on a rail with a brand new process.
There will be no slow motion or still life of Roy
Wilkens strolling through Watts in a Red, Black and
Green liberation jumpsuit that he had been saving
For just the proper occasion.
Green Acres, The Beverly Hillbillies, and Hooterville
Junction will no longer be so damned relevant, and
women will not care if Dick finally gets down with
Jane on Search for Tomorrow because Black people
will be in the street looking for a brighter day.
The revolution will not be televised.
There will be no highlights on the eleven o'clock
news and no pictures of hairy armed women
liberationists and Jackie Onassis blowing her nose.
The theme song will not be written by Jim Webb,
Francis Scott Key, nor sung by Glen Campbell, Tom
Jones, Johnny Cash, Englebert Humperdink, or the Rare Earth.
The revolution will not be televised.
The revolution will not be right back after a message
bbout a white tornado, white lightning, or white people.
You will not have to worry about a dove in your
bedroom, a tiger in your tank, or the giant in your toilet bowl.
The revolution will not go better with Coke.
The revolution will not fight the germs that may cause bad breath.
The revolution will put you in the driver's seat.
The revolution will not be televised, will not be televised,
will not be televised, will not be televised.
The revolution will be no re-run brothers;
The revolution will be live.
|
|
|
|
|